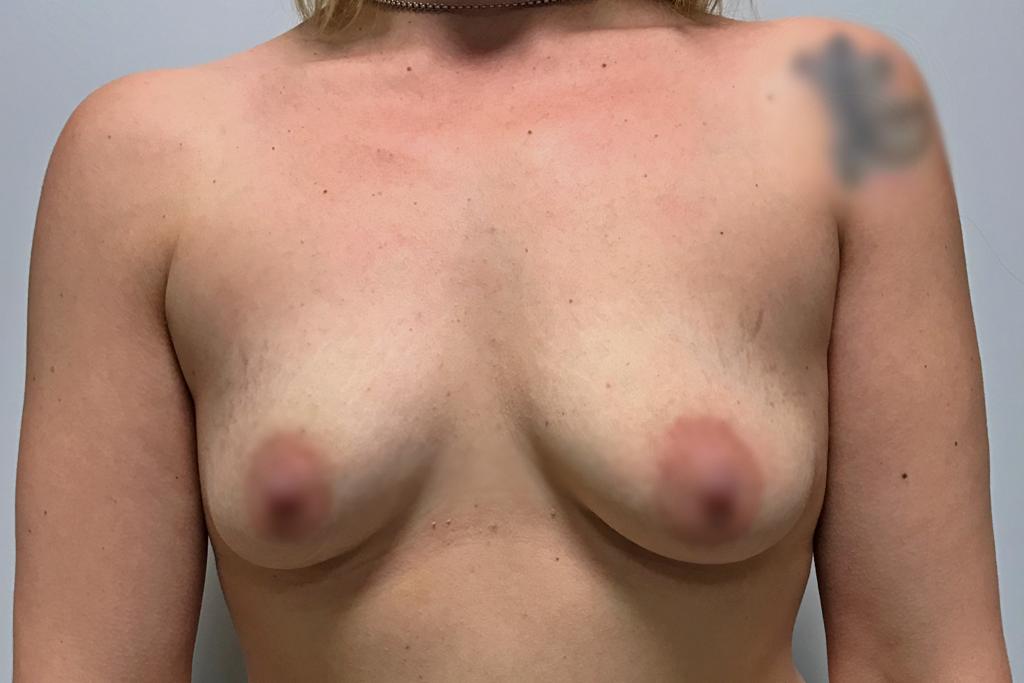
Breast hypoplasia is defined by a volume of breasts that are insufficiently developed in relation to the patient’s body. It can be the consequence of an insufficient development of the gland at puberty, or appear secondarily by loss of glandular volume (pregnancy, weight loss, hormonal disturbances).
There are two forms of prostheses, round, ensuring a beautiful neckline, or anatomical, for a more natural rendering of the breast. The breast can be reassembled at the same time, if necessary.
To obtain a natural result, it will be necessary to consider the initial volume of the breast as well as its shape before the installation of the breast implants.
This procedure is performed under general anesthesia, on an outpatient basis. The access routes are generally either in the lower periareolar, or under the mammary, or axillary. The position of the implant will be either premusculary, where the prostheses are placed directly behind the gland, in front of the pectoral muscles; either retromusculary, where the prostheses are placed deeper, behind the pectoral muscles.
The aftermath can sometimes be painful the first few days, especially when the implants are large and especially if they are placed behind the muscles. Waterproof dressings for taking a shower are in place, as well as a compression bra to keep day and night. Consideration should be given to a recovery with a break in activity lasting 5 to 10 days. It is advisable to wait 1 to 2 months to resume a sporting activity.
Pregnancy and breastfeeding are possible after such an intervention, but it is better to wait a year.
GREASE TRANSFER IN CASES OF BREAST AUGMENTATION FOR AESTHETIC VIEWS OR FOR CONGENITAL DEFORMATIONS
The injection of fat into the breasts increases the volume of the breast in a natural way, without breast prostheses and without scar. This fat transfer technique at breast level is currently recognized as being very effective.
This technique consists of removing fat from the overloaded areas (belly, hips, inner side of the knees, thighs), which will be centrifuged and then reinjected into the breasts. It therefore allows an increase in the volume of the breast, certainly moderate, but completely natural, without foreign body, and not giving the appearance of an artificial breast. And, it allows at the same time to treat at the same time any localized fat overloads (fat sampling sites).
The operation is performed under general anesthesia, on an outpatient basis. Edema and bruising can appear in the areas of the sample and generally resolve within 10 to 20 days after the procedure.
The result is appreciated within 3 to 6 months. A second session is possible a few months later if necessary (and if this is possible given the fat-giving areas) in order to further increase the volume of the breasts, or to improve their shape.
Breast Surgery
BREAST HYPERTROPHY SURGERY
Breast enlargement corresponds to an excessive volume of the breasts causing aesthetic and functional discomfort (back pain, difficulty dressing) as well as a real psychological impact. Excess volume is usually associated with sagging breasts (breast ptosis) and sometimes asymmetry.
The aim of the intervention is to reduce the volume of the breasts, the correction of the ptosis and any asymmetry, in order to obtain two breasts that are harmonious in relation to the patient’s body (two reduced, ascended, symmetrical and reshaped breasts).
The breast reduction procedure is always done under general anesthesia and very often requires an overnight stay.
At the end of the intervention, a shaping dressing is made and a bra is put in place ensuring good compression. Wearing a bra is recommended for about a month.
The postoperative operations are generally not very painful. Swelling (edema) and bruising (bruising) of the breasts, as well as discomfort in raising the arms are commonly seen. Consideration of convalescence and work stoppage lasting 8 to 21 days. We recommend waiting one to two months before resuming a sporting activity.
The result of this intervention can only be judged from one year after the intervention. You just have to have the patience to wait for the time needed to reduce the scarring.
Beyond the local improvement, this intervention has a favorable impact on the balance of weight, the practice of sports, the clothing possibilities and the psychological state.
LIFTING OF THE BREASTS (MASTOPEXIA) OR SURGERY OF THE BREAST PTOSE
Breast ptosis is defined by sagging breasts and distension of the surrounding skin. This phenomenon, which increases with age, also occurs after significant weight loss or pregnancy.
We can observe a breast ptosis in the context of a breast that is too small which can then be compensated by the installation of breast prostheses.
The aim of the intervention is to put the areola and the nipple in the right position, to refocus and ascend the mammary gland and to remove the excess skin.
This procedure takes place under general anesthesia and most often on an outpatient basis. It induces scars, in inverted T (periareolar around the areola, vertical between the lower pole of the areola and the furrow under the breast, horizontal hidden in the furrow under the breast). In the case of a moderate ptosis it is possible to remove the transverse scar in the groove under the breast.
The aftermath is not very painful. Swelling (edema) and bruising (bruising) of the breasts as well as discomfort in raising the arms are commonly seen.
The dressing change is performed after 24 hours and will be repeated regularly until complete healing. The wearing of a bra ensuring good support is indicated for about a month, night and day. Consider recuperation and work stoppage for 7-10 days and wait one to two months to resume a sporting activity.
The result can only be judged from one year after the intervention; the chest then most often has a harmonious and natural curve, symmetrical or very close to symmetry.
Beyond local improvement, this intervention generally has a favorable impact on weight balance, sports, clothing and psychological state.
THE INVAGINATION OF THE NIPPLE
The invaginated nipple is retracted on itself, inside the breast, in the breast areola,
The aim of the intervention is to restore a central relief to the nipple, by cutting the milk ducts deep under the nipple, to allow its emergence.
This gesture is performed under local anesthesia, on an outpatient basis. This intervention leaves a minimal scar ransom and in general very little visible.
Dressings are expected for a fortnight until the son is removed.
The final projection of the nipple is appreciated at around 1 year.
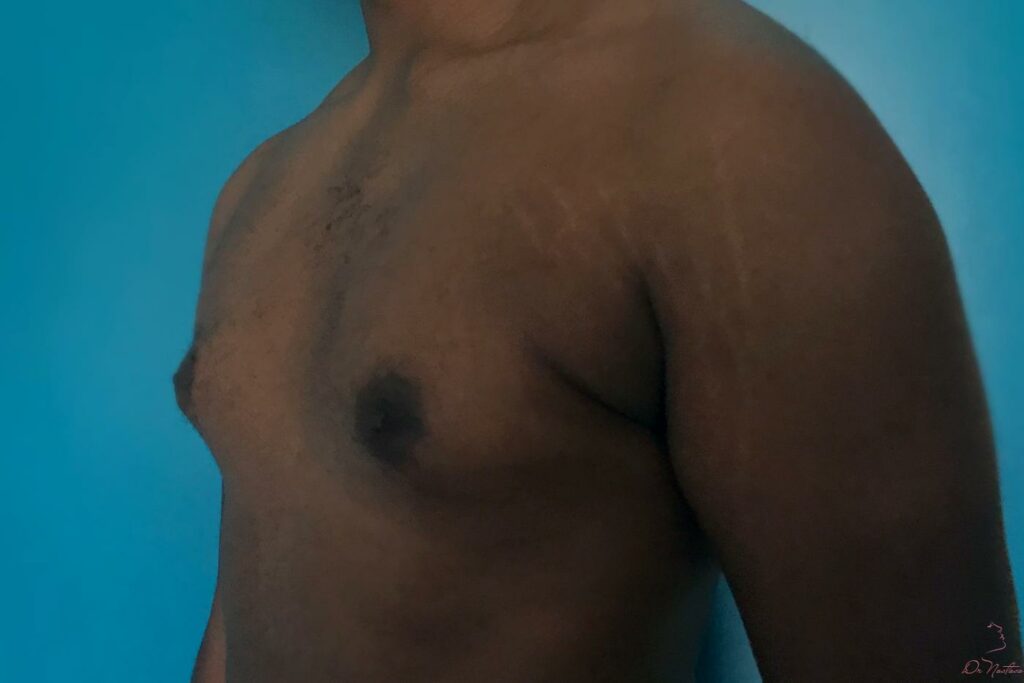
GYNECOMASTIE
Gynecomasty is defined by an increase in the volume of the mammary gland in males. It can be united or bilateral. In some cases, it may be related to abnormal hormone production.
Increased breast volume in men, especially during adolescence, is often frowned upon and can cause many psychological problems.
The intervention, under general anesthesia, on an outpatient basis, aims to reduce the breast volume by direct surgical excision (subcutaneous mastectomy) for glandular forms, or by liposuction for fatty forms.
During the intervention, a drain can be installed depending on the technique used. This drain is used to evacuate the blood and lymphatic residues which could accumulate at the level of the operating site. At the end of the intervention, a shaping dressing is made with an elastic bandage.
The aftermath can sometimes be painful the first few days. In case of isolated liposuction, the patient may locally experience pain such as “strong aches”. Edema (swelling), bruising (bruising) and discomfort in raising the arms are common in the early stages.
The first dressing is removed after a few days and is replaced by a lighter dressing associated with the wearing of a bolero, to be worn day and night for a certain time.
The total time off work ranges from five to twenty-one days. It is advisable to wait one to two months before resuming a sporting activity.
A period of two to three months is necessary to assess the final result. The decrease in breast volume provides physical comfort, especially when dressing. The result is often very beneficial on the psychological level because a gynecomasty is often considered as a shadow of manhood.
BREAST RECONSTRUCTION
Mastectomy is the removal of the mammary gland, a spindle of the skin and the areola. Unfortunately, it remains necessary in certain forms of breast cancer.
A request for breast reconstruction is completely legitimate after a mastectomy.
There are different possibilities for breast reconstruction depending on the patient’s body, wishes and whether or not she has had radiation therapy.
Breast reconstruction by prosthesis
When the quality of the skin and the underlying pectoral muscle are satisfactory, the simplest mode remains reconstruction by prosthesis. It can be preceded by a period of tissue expansion if the amount of skin is insufficient.
Reconstruction with a large back flap
This technique is used when the residual skin is insufficient or weakened by the rays, and cannot by itself protect an internal prosthesis. The intervention aims to reconstruct the volume and contours of the breast by a spindle of skin and muscle taken from the back region. An internal prosthesis can complete the reconstruction, as well as a reconstruction of the areola and nipple, and possibly an intervention on the contralateral breast to improve symmetry.
Right abdominal reconstruction
The aim of this technique is to reconstruct the volume and contours of the breast by transferring excess skin and fat from the abdominal sub-umbilical region to the thorax. The technique gives the reconstructed breast a relatively natural shape and flexibility since it consists of the patient’s own tissues. A reconstruction of the areola and the nipple and possibly an intervention on the other breast to improve symmetry can complete the reconstruction by straight line of the abdomen.
Breast reconstruction is never compulsory and does not in any way affect oncology surveillance.
Contact
Schedule an appointment now and get the look you desire with our plastic surgery service.